
Plantar fasciitis is one of the most common causes of heel and arch pain, especially among athletes, runners, active adults, and people who spend long hours on their feet. While the condition can be extremely frustrating, it is also highly treatable with the right combination of hands-on care, movement correction, and supportive strategies.
What is the Plantar fascia?
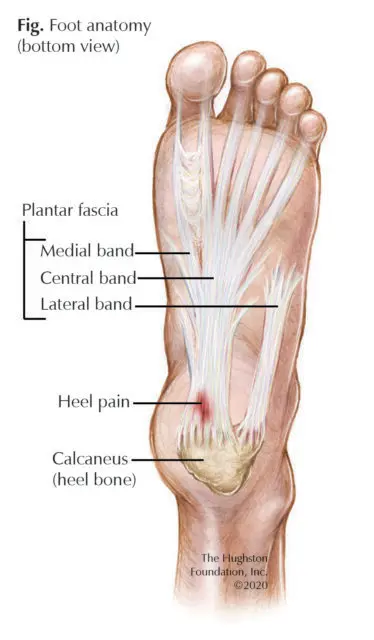
The plantar fascia is a thick, durable band of connective tissue that spans the bottom of your foot. It runs from the calcaneus (heel bone) to the forefoot, where it helps maintain the shape and stability of the arch. Rather than being a single sheet, the plantar fascia is made up of three distinct bands named the medial, central, and lateral bands.
What is Plantar Fasciitis?
Despite the name plantar fasciitis, this condition is not primarily an inflammatory disorder. Current research shows that the plantar fascia typically undergoes degenerative changes, similar to what is seen in chronic tendinopathies (2). For this reason, many clinicians now use the term “plantar fasciopathy” or “plantar heel pain” to better reflect the underlying biology.
These degenerative changes occur when the tissue is overloaded beyond its current capacity, leading to micro-damage, disorganization of collagen fibers, and reduced tissue stiffness—rather than the classic inflammatory response implied by “-itis.” Trojian & Tucker (2019) highlighted this shift in understanding, aligning plantar fasciopathy with conditions such as Achilles tendinopathy or lateral epicondylopathy (tennis elbow).
This distinction is important because it changes how we treat the condition. Instead of focusing on anti-inflammatory approaches alone, modern evidence supports treatments that address the tissue’s ability to tolerate load, including strengthening, progressive loading, and biomechanical interventions.
Who Gets Plantar Fasciitis?
Plantar fasciitis affects roughly one in ten people and is most commonly seen in two seemingly opposite populations—highly active individuals and those with more sedentary lifestyles. Endurance athletes, especially runners, place repetitive and sometimes rapidly increasing loads on the plantar fascia, which can exceed the tissue’s ability to adapt and repair. Conversely, individuals with lower activity levels and higher BMI often experience plantar fasciitis because the fascia is exposed to greater mechanical demand despite having reduced tissue capacity (2). Although these groups differ, they share a common underlying issue: the load placed on the plantar fascia surpasses its ability to tolerate that load. Whether due to increased training volume or decreased tissue resilience, this mismatch between load and capacity helps explain why plantar fasciitis develops and guides treatment strategies centered on restoring strength, improving tissue tolerance, and adjusting daily or athletic demands.
Do I Have Plantar Fasciitis?
Plantar fasciitis typically presents with a very recognizable pattern of symptoms, the most classic being sharp, localized heel pain with the first few steps after a period of rest—especially in the morning. Many people describe the initial steps as almost unbearable, followed by gradual improvement as they move around and the tissue warms up. However, symptoms often return or worsen toward the end of the day as the plantar fascia becomes fatigued. Another common clue is the recent start or increase of a weight-bearing activity, such as training for a first 5K, beginning a new job that requires prolonged standing, or walking significantly more than usual. This combination of morning pain, pain after inactivity, improvement with movement, and a recent change in load or activity strongly points toward plantar fasciitis.
Is Imaging Necessary?
Imaging is not always required to diagnose plantar fasciitis, as the condition is primarily identified through clinical history and physical examination (3). However, imaging can be useful when symptoms are atypical or when it is important to rule out other causes of heel pain. X-rays provide information about the bone structure and can help exclude fractures or identify heel spurs, though heel spurs are only loosely associated with plantar fasciitis, with studies showing that only about half of individuals with a spur experience plantar fascia pain. Ultrasound offers a quick, cost-effective way to evaluate the thickness and integrity of the plantar fascia, making it an excellent first-line imaging choice. MRI provides the most detailed view of soft tissues and can help identify alternative diagnoses, such as nerve entrapments or deeper soft-tissue pathology, but it is typically reserved for persistent or unclear cases due to higher cost and longer imaging times. At M3 Chiropractic & Sports Medicine, we utilize diagnostic ultrasound in-office to efficiently confirm findings and guide the most appropriate treatment plan.
Here at M3 Chiropractic and Sports Medicine, we can utilize diagnostic ultrasound to quickly and cost-effectively assess the plantar fascia. After the diagnosis is confirmed, we can be sure of what treatment would be most effective and appropriate.
Prognosis
Research provides both encouraging and challenging news regarding the outlook for plantar fasciitis. The encouraging aspect is that this condition is generally self-limiting, meaning that most individuals experience full resolution of symptoms over time without requiring invasive intervention.
However, the timeline for recovery can be lengthy. Many people improve significantly within 12 to 24 months, but some studies indicate that a subset of patients may continue to experience intermittent symptoms for several years—occasionally up to a decade. This subset of patients luckily report very low pain levels and minimal little functional limitations (4).
While this may sound discouraging, it’s important to remember that symptoms typically become far more manageable with appropriate treatment, load management, and targeted rehabilitation. Most patients regain full function and return to the activities they love long before complete resolution is documented.
Treatments
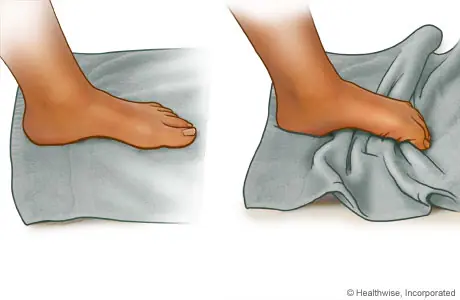
Current research consistently shows that the most effective long-term treatment for plantar fasciitis centers on improving the foot’s ability to tolerate load through targeted strengthening. This includes exercises for the intrinsic foot muscles as well as the supporting musculature of the toes, arch, and calf (5,6). Foundational movements such as:
- Short Foot exercise
- Towel Scrunch exercise (left picture)
- Toe raises
- Calf raises (right picture)

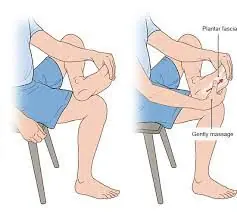
While strengthening builds long-term resilience, short term symptom management is also important. Manual therapy to the foot, ankle, and posterior chain can temporarily decrease pain and improve mobility. Gentle stretching of the plantar fascia and calf complex, as well as icing after activity, can help manage flare-ups. For individuals who experience severe pain with their first steps in the morning, performing light foot mobility or gentle calf stretches before getting out of bed may lessen that initial discomfort (5).
Extracorporeal Shockwave Therapy (ESWT)
In addition to exercise-based care, Extracorporeal Shockwave Therapy (ESWT) has strong support in the current literature as an effective adjunct treatment. Studies show that ESWT can significantly reduce pain and improve function, especially when combined with a structured loading program (7). This combined approach enhances tissue remodeling and can accelerate recovery for individuals with persistent or stubborn symptoms.
At M3 Chiropractic & Sports Medicine, we frequently incorporate ESWT alongside individualized rehabilitation to address both pain and the underlying mechanical deficits contributing to plantar fascia overload.
For more on Extracorporeal Shockwave therapy check out our blog!
Our Holistic Approach to Plantar Fasciitis at M3 Chiropractic & Sports Medicine
At M3 Chiropractic & Sports Medicine, we take a comprehensive and individualized approach to treating plantar fasciitis. By combining our clinical expertise with an understanding of your daily activities, training demands, and lifestyle factors, we create a personalized treatment plan that targets the root cause of your heel and foot pain. Our goal is to not only provide effective short-term relief, but also promote long-term healing and durability so you can move with confidence.
Whether you’re dealing with persistent morning heel pain, limitations during activity, or recurring flare-ups, our team is ready to guide your recovery. When you’re prepared to restore your mobility, reduce pain, and return to your normal activities, we’re here to help you achieve lasting comfort and optimal foot function.
References
- Stecco C, Corradin M, Macchi V, Morra A, Porzionato A, Biz C, De Caro R. Plantar fascia anatomy and its relationship with Achilles tendon and paratenon. J Anat. 2013 Dec;223(6):665-76. doi: 10.1111/joa.12111. Epub 2013 Sep 12. PMID: 24028383; PMCID: PMC3842207.
- Trojian T, Tucker AK. Plantar Fasciitis. Am Fam Physician. 2019 Jun 15;99(12):744-750. PMID: 31194492.
- Kirkpatrick J, Yassaie O, Mirjalili SA. The plantar calcaneal spur: a review of anatomy, histology, etiology and key associations. J Anat. 2017 Jun;230(6):743-751. doi: 10.1111/joa.12607. Epub 2017 Mar 29. PMID: 28369929; PMCID: PMC5442149.
- Hansen L, Krogh TP, Ellingsen T, Bolvig L, Fredberg U. Long-term prognosis of plantar fasciitis: a 5-to 15-year follow-up study of 174 patients with ultrasound examination. Orthopaedic journal of sports medicine. 2018 Mar 1;6(3):2325967118757983
- Boob MA Jr, Phansopkar P, Somaiya KJ. Physiotherapeutic Interventions for Individuals Suffering From Plantar Fasciitis: A Systematic Review. Cureus. 2023 Jul 31;15(7):e42740. doi: 10.7759/cureus.42740. PMID: 37654968; PMCID: PMC10467524.
- Huffer D, Hing W, Newton R, Clair M. Strength training for plantar fasciitis and the intrinsic foot musculature: A systematic review. Phys Ther Sport. 2017 Mar;24:44-52. doi: 10.1016/j.ptsp.2016.08.008. Epub 2016 Aug 18. PMID: 27692740.
- Charles R, Fang L, Zhu R, Wang J. The effectiveness of shockwave therapy on patellar tendinopathy, Achilles tendinopathy, and plantar fasciitis: a systematic review and meta-analysis. Front Immunol. 2023 Aug 16;14:1193835. doi: 10.3389/fimmu.2023.1193835. PMID: 37662911; PMCID: PMC10468604.