
What is it?
Femoroacetabular Impingement (FAI) is a term used to describe a pinching sensation felt deep in the hip joint. “Femoroacetabular” refers to the two parts of the hip — the femur (thigh bone) and the acetabulum (hip socket). “Impingement” simply means that these two surfaces are coming into contact in a way that creates irritation or pinching.
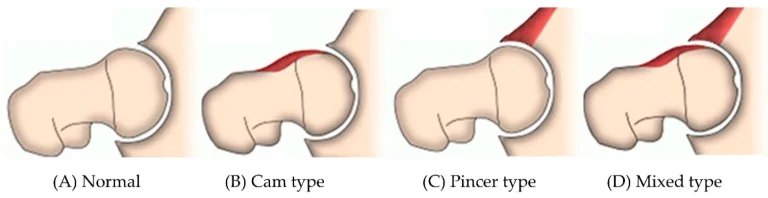
This pinching can happen when there is extra bone growth on (1):
- The neck of the femur (called a cam deformity) (B)
- The rim of the acetabulum, or socket (called a pincer deformity) (C)
- Or a combination of both (called a mixed deformity, which is the most common) (D)
Because of these shape differences, the ball and socket may not move as smoothly during certain motions. The pinch is most commonly felt with deep hip flexion (bringing your knee toward your chest), squatting, or hip internal rotation. All deformities present with the same symptoms, therefore imaging is needed to determine the type. These bony overgrowths are mainly due to genetic differences, but can be brought on by lifestyle factors like increased time spent at end ranges of motion. The people that might spend a lot of time at the end ranges may include baseball catchers, gymnasts, and even some trade workers.
It’s important to know that many people have these bony changes and never experience pain. The presence of imaging findings does not automatically mean you will have symptoms (2).
How to Know If You Have FAI?
A true diagnosis of Femoroacetabular Impingement (FAI) involves both your symptoms and imaging findings, such as an X-ray or MRI. FAI is not diagnosed from a scan alone. To make the diagnosis, there must be a combination of symptoms, signs, and imaging findings. Fortunately, the rehab process is very similar if you have true FAI or if you are just experiencing a tight and painful hip. Therefore, rehab does not have to wait for any images to be taken.
Symptoms
Common symptoms of FAI include (3):
- Deep pain in the front of the hip or groin
- A feeling of tightness in the joint
- Pain with squatting or bringing the knee toward the chest
- Discomfort with prolonged sitting
- Pain may also refer to the outside of the hip or even the lower back
- Some people report popping, clicking, or catching sensations in the hip joint.
Signs
Signs are findings that a medical professional observes during an exam. A medical professional will perform a series of tests to help determine whether your symptoms are coming from inside the hip joint.
These signs may include:
- Reduced hip range of motion (especially internal rotation)
- Positive orthopedic tests such as FADIR and FABER (4)
- Restriction or limitations during the Hip Scour test
Imaging
Imaging helps to confirm the type of FAI by identifying cam, pincer, or mixed bone changes. However, imaging findings do not always match symptoms. Some people have clear bony overgrowth and no pain at all. Others may have hip pain despite minimal structural changes.
That’s why diagnosis is based on the full picture of your symptoms, your exam findings, and imaging when appropriate.
How FAI Affects Your Hip Over Time
The bony shape changes seen with cam or pincer morphology can alter how forces move through the hip joint. Over time, this may increase stress on the labrum (the ring of cartilage around the socket) and the joint surface itself. Research shows that because of the bony changes people with significant cam or pincer changes have a higher risk of developing labral tears and hip osteoarthritis compared to those without these changes (5).
However, it’s important to understand that increased risk does not mean inevitable damage. Many people with these structural findings never develop arthritis or ongoing pain (6). Factors such as activity level, strength, movement control, and overall joint health all play an important role in how the hip tolerates load over time.
Conservative Management
In hips with FAI — and even in cases where labral tears or early osteoarthritis are present — conservative treatment is often very effective. The foundation of conservative care is building hip strength and stability, particularly through the glutes and surrounding musculature. In individuals with FAI, strength is often more beneficial than aggressive stretching, especially stretching into positions that reproduce the pinch. Stronger muscles help the joint better tolerate load and move more efficiently.

Exercises may include:

- Glute bridges
- Romanian deadlifts
- Copenhagen planks
- Monster walks
- Step-ups
Exercise modifications are also important. For example, if a traditional squat causes pinching, elevating the heels or adjusting stance width can reduce the amount of hip flexion required and make the movement more comfortable. Small changes in positioning can make a significant difference.
Core stability and pelvic control are also essential. Pelvic positioning directly influences how the femur sits in the socket. Improving control of pelvic tilt can enhance hip mechanics and reduce irritation.
Manual therapies such as spinal or extremity manipulation and soft tissue work can help reduce pain and temporarily improve mobility. These techniques are most effective when used to support a structured strengthening program, not replace it.
While most people improve with conservative management, there are cases where symptoms persist despite a well-designed rehab program. In those situations, surgical options may be considered. At M3 Chiropractic and Sports Medicine, we recommend starting with conservative care first. In many cases, improving strength, control, and load tolerance is enough to return patients to the activities they enjoy.
Surgical Options
The most common procedure for FAI is hip arthroscopy, a minimally invasive surgery that reshapes the areas of extra bone causing impingement. Surgeons may also repair or address damage to the labrum (1).
Hip arthroscopy can improve range of motion and relieve pain for many patients. However, long-term improvements in pain and function are often similar to what can be achieved with structured physical therapy (7,8).
Surgery can be helpful — particularly for patients whose symptoms persist despite conservative care, or those with specific structural variants — but it is not automatically superior to rehabilitation. For most individuals, conservative management is recommended first.
For information on more invasive surgeries, visit: https://doi.org/10.1093/jhps/hnae034.
Should I get surgery?
The decision to have surgery is a personal decision that depends on multiple factors, including:
- How much pain or limitation you are experiencing
- Your response to conservative rehabilitation
- Your activity goals and lifestyle demands
- Your tolerance for surgical risk and recovery time
- The financial and time commitment involved
Surgery carries potential risks, including complications and the need for post-operative rehab. While it may improve joint mechanics and range of motion, it does not guarantee better long-term pain relief or function for everyone.
For some patients, guided rehabilitation alone is enough to return to the activities they enjoy. For others, persistent symptoms despite months of structured care may make surgery a reasonable next step. The key is making an informed choice based on your symptoms, goals, and response to treatment — not just imaging findings.
What is the bottom line?
If you think you may have FAI and are experiencing hip pain, it is important to get evaluated by a healthcare professional. Proper guidance can help you return to normal activities and prevent long-term issues.
Remember:
- Modify, don’t avoid exercises
- Emphasize strength over aggressive stretching
- Surgery is not always superior to well-structured conservative care
- The pain you are experiencing now does not have to be permanent.
If you are experiencing persistent hip pain or pinching with movement, a proper evaluation is important. So, schedule an evaluation with Dr. Drew and Dr. Paul to receive personalized guidance and a plan to safely return to your normal self.
References:
- Fernando Gómez-Verdejo, Elsa Alvarado-Solorio, Carlos Suarez-Ahedo, Review of femoroacetabular impingement syndrome, Journal of Hip Preservation Surgery, Volume 11, Issue 4, December 2024, Pages 315–322, https://doi.org/10.1093/jhps/hnae034
- Laborie LB, Lehmann TG, Engesæter IØ, Eastwood DM, Engesæter LB, Rosendahl K. Prevalence of radiographic findings thought to be associated with femoroacetabular impingement in a population-based cohort of 2081 healthy young adults. Radiology. 2011 Aug;260(2):494-502. doi: 10.1148/radiol.11102354. Epub 2011 May 25. PMID: 21613440.
- Clohisy JC, Knaus ER, Hunt DM, Lesher JM, Harris-Hayes M, Prather H. Clinical presentation of patients with symptomatic anterior hip impingement. Clin Orthop Relat Res. 2009 Mar;467(3):638-44. doi: 10.1007/s11999-008-0680-y. Epub 2009 Jan 7. PMID: 19130160; PMCID: PMC2635448.
- Ratzlaff, C., Simatovic, J., Wong, H., Li, L., Ezzat, A., Langford, D., Esdaile, J.M., Kennedy, C., Embley, P., Caves, D., Hopkins, T. and Cibere, J. (2013), Reliability of hip examination tests for femoroacetabular impingement. Arthritis & Rheumatism, 65: 1690-1696. https://doi.org/10.1002/acr.22036
- Neumann G, Mendicuti AD, Zou KH, Minas T, Coblyn J, Winalski CS, Lang P. Prevalence of labral tears and cartilage loss in patients with mechanical symptoms of the hip: evaluation using MR arthrography. Osteoarthritis Cartilage. 2007 Aug;15(8):909-17. doi: 10.1016/j.joca.2007.02.002. Epub 2007 Mar 26. PMID: 17383908.
- Register B, Pennock AT, Ho CP, Strickland CD, Lawand A, Philippon MJ. Prevalence of abnormal hip findings in asymptomatic participants: A Prospective, Blinded Study: A Prospective, Blinded Study. The American Journal of Sports Medicine. 2012;40(12):2720-2724. doi:10.1177/0363546512462124
- Palmer A, Fernquest S, Rombach I FAIT Study Group, et al. Medium-term results of arthroscopic hip surgery compared with physiotherapy and activity modification for the treatment of femoroacetabular impingement syndrome: a multi-centre randomised controlled trial. British Journal of Sports Medicine 2025;59:109-117.
- Mansell NS, Rhon DI, Meyer J, Slevin JM, Marchant BG. Arthroscopic surgery or physical therapy for patients with femoroacetabular impingement syndrome: a randomized controlled trial with 2-year follow-up. Am J Sports Med. 2018 May;46(6):1306-1314. doi: 10.1177/0363546517751912. Epub 2018 Feb 14. PMID: 29443538.